Physiological Regulation Through Manual Therapy
ERIC A. MEIN, MD
From the Meridian Institute Virginia Beach, Virginia (EAM, DGR,DLM,CDN)
and
[NOTE: This book chapter was published in Physical Medicine and Rehabilitation:
State of the Art Reviews, Vol. 14, No. 1, February, 2000. Philadelphia,
Hanley & Belfus, Inc.; see
below for continuing
education credit for this material.]
CORRECTION AND REGULATION Manual therapy can be divided into two distinct conceptual
approaches to treatment: specific adjustments for correction of anatomic
issues (structure) and adjustments for physiologic regulation (function).
In recent years, the primary emphasis of most practitioners has been on
finding structural problems associated with musculoskeletal issues and
correcting anatomic findings ("lesions" and "subluxations"). Less
emphasized has been the capability for manual therapy to regulate physiology,
Recognition of the structure versus function choices within manual therapy dates to the early days of osteopathy. For example, Hazzard (1899), a prominent early osteopathic physician, acknowledges both of these approaches in his textbook Principles of Osteopathy: In our treatment of a spine there are two points which we may take into consideration; two objects which we may have in view. In the first place, we may wish to TREAT THE SPINE ITSELF [anatomical correction. In the second place, we may wish to REACH, BY TREATING THE CENTERS ALONG THE SPINE, THE VISCERA TO WHICH THESE NERVES RUN [physiologic regulation]. It is not always possible to disassociate these in your practice.23The textbooks of the early 1900s emphasized regulation, 2,5,11,19,23,30a,51,60 yet by 1991, Kuchera and Kuchera state: "The majority of DOs do not use manipulation. Many of those physicians who do so use it primarily for treating musculoskeletal complaints. They do not use manipulation for its homeostatic benefits [regulation] to the body's physiology."30 Johnston points out that there are aspects of osteopathic manipulation in which spinal segment dysfunction is not necessarily the focus for diagnosis and treatment.25 These include direct manipulation of the visceral organs themselves, influencing cerebrospinal fluid flow, and adjustment of postural influences on visceral support systems. All of these are interventions that regulate physiology. The general lack of awareness of regulatory techniques
and effects can complicate the interpretation of research. For example,
Balon et al. compared active and simulated chiropractic manipulations as
an adjunctive treatment for childhood asthma.4 They concluded
that, because there were no significant differences in response to the
active and simulated treatments, chiropractic spinal manipulation provides
no benefit. However, the so-called simulated or sham treatment involved
"soft tissue manipulation and gentle palpation to the spine, paraspinal
muscles, and shoulders." Additional manipulations were applied to the head,
ankles and feet, gluteal region, and occipital protuberance. "Low-amplitude,
low-velocity impulses were applied in all these nontherapeutic contacts,"
in contrast to the standard high-velocity chiropractic manipulation.
Unfortunately, this simulated treatment resembles a traditional general
osteopathic regulatory treatment.5,17,23 The Early American
Manual Therapy website provides easy access to several such examples from
the traditional manual therapy literatures.32
Figure
1, which dates back to 1909, demonstrates such a technique. In
the Balon study, both treatments produced positive effects. The authors
note, "We are unaware of published evidence that suggests that positioning,
palpation, gentle soft-tissue therapy, or impulses to the
Despite the low level of awareness, there is a substantial body of regulatory technique in historical materials, and there are osteopaths still very much concerned with this aspect of manual therapy.30 There is also a strong linkage between this broader approach to manual medicine and the growing interest in complementary and alternative medicine. Edgar Cayce, to whom the Journal of the American Medical Association traced the roots of modem day holism,10 strongly advocated osteopathy as a very helpful treatment system, especially for maintaining coordination of the nervous system. Cayce indicated the osteopathy is "not merely the punching in a certain segment or the cracking of the bones, but is the keeping of a balanceby the touch-between the sympathetic and the cerebrospinal system! That is real osteopathy!"36 One approach, used by the Kucheras, groups systems of the body by their common autonomic and lymphatic elements.30 It explores selected structural and functional considerations in osteopathic medicine, with an emphasis on physiology and reflexes. The goal is to enhance the body's homeostatic mechanisms. Their book discusses a variety of techniques and clinical experience of effectiveness, for each system of the body. The Kucheras provide techniques to enhance circulation and drainages. Each section discusses (1) sympathetic and parasympathetic innervation and relevant reflexes, (2) lymphatic drainage patterns, and (3) manipulative treatment for influencing sympathetic, parasympathetic, and lymphatic drainage to augment homeostasis. In this chapter, we address four key concepts affecting
regulation: coordination, centers, reflexes, and drainage. We draw
on the historical osteopathic and chiropractic literature for techniques
and examples and review research that demonstrates the effectiveness and
explores the mechanisms of these techniques.
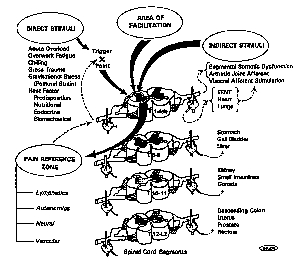
FOUR KEY CONCEPTS: REFLEXES, COORDINATION, CENTERS, AND DRAINAGE Reflexes To go beyond diagnosing and treating musculoskeletal complaints and to treat the entire person, manual medicine requires the existence of physiologic linkages between the surface/somatic areas and the deeper viscera. These reflex connections exist in the form of viscerosomatic reflexes, in which dysfunction in the viscera is expressed as somatic dysfunction, and somatovisceral reflexes, in which dysfunction or treatment at the surface of the body is reflexively conveyed to the viscera.54 Furthermore, the spinal cord behaves as a "neurologic lens" for a variety of stressors and acts as an "organizer" of disease and dysfunctional processes that initiates both somatic and visceral Symptoms.28 This is illustrated in Figure 2. Although the locations of many of the centers are
obviously correlated with the segmental anatomy of the body, there also
exist reflexes that may cut across segmental boundaries and affect areas
far removed from the point of manipulation. "Referred pain" is one
obvious form of a viscerosomatic reflex. For example, gallbladder
dysfunction is often experienced as muscle pain in the right shoulder.
There is a direct relationship between certain segments of the spine and
various internal organs (Table 1). Diagnosis
in osteopathy can rely heavily on viscerosomatic reflexes. While
the primary focus here is on physiologic regulation through somatovisceral
reflexes, it is worth noting the evidence for viscerosomatic reflexes,
because it provides a feedback mechanism for the practitioner, and diagnosis
and treatment are often carried out simultaneously. Beal reviews
the clinical and
Somatovisceral reflexes have received little attention
yet are significant for physiologic regulation. Among the more important
reflexes for regulation of physiology are Chapman's reflexes. In
the late 1930s, Frank Chapman, D.O., first published his findings identifying
specific neurolymphatic reflex points that correspond to particular organs
and glands. There is a discussion of the diagnostic and therapeutic
application of Chapman's reflexes in the text An Endocrine Interpretation
of Chapman's Reflexes.43 Most of these points are
located on the front of the body between the ribs next to the sternum and
on the back along the spine between the spinous processes and the tips
of the transverse processes. Palpation of Chapman's points can be
used for assessment of lymphatic function with correlation to specific
organs. Stimulation of Chapman's points can influence the
Patriquin gives practical guidelines for diagnosis
and treatment using Chapman's reflexes.45 For example,
for irritable bowel syndrome, Chapman's reflexes for the colon are found
along the anterior aspect of the iliotibial bands, a 2inch strip on the
lateral side of each thigh. The anatomic location of the reflex ganglioform
masses found can be correlated with specific portions of the colon.
These can be treated with soft tissue kneading, a mechanical percussion
hammer, or other types of vibration to
Some of the Chapman's points bear an obvious segmental relationship to the target organ. For example, the anterior point for bronchitis is the intercostal space between the second and third rib close to the sternum. The posterior point is located at the second dorsal (thoracic) vertebra, midway between the spinous process and the tip of the transverse process.43 On the other hand, some of the Chapman's points bear little obvious relation to the target organ. For example, the anterior points for the eye problems of retinitis and conjunctivitis are located on the front of the humerus.43 It is not clear how Chapman's reflexes actually work
physiologically. Some have a segmental relationship, but some are
aberrant (e.g., the eye-humerus reflex cited above). Patriquin is
uncomfortable relating Chapman's reflexes to autonomic responses, because
in his view, the autonomics, by the time they reach the surface, tend to
be quite diffuse (the thermodiagnosis
Despite the unclear anatomic justification for Chapman's
reflexes, there is a solid experimental physiologic basis for regulation
of visceral function by manual surface stimulation and inhibition.
Sato explored somatic-autonomic reflexes in animals.54
Sato and his colleagues, working with anesthetized animals, traced reflexes
from various types of mechanical, thermal, and chemical
Coordination The body's physiologic processes normally operate
in a coordinated manner, and the goal of manual therapy is to restore coordination.
For example, Gregory (1922) equated coordination with health and incoordination
with disease: "It is the existence and continuation of the normal equilibrium,
and of perfect coordination and reflex action, which maintain perfect health,
and it is the existence of some variation and loss of the perfect equilibrium
of nerve action which engenders derangement
Modern systems theory, when combined with the concept of energy, leads to the prediction that the various parts of the body may interact not only physiologically, but also energetically and therefore informationally.57 This interaction can reach the level of harmonic integration, which has been termed entrainment.33 How, then, does manual therapy accomplish coordination? Two techniques bear mentioning. First, physiologic regulation and coordination are accomplished through stimulation and inhibition of centers along the spine and at other locations on the surface of the body. Goetz defines the two types of manipulation that regulate physiology: stimulation and inhibition.17 To stimulate is to manipulate the parts thoroughly. To inhibit is to desensitize or hold the part for 1-3 minutes. According to Ashmore, "Stimulation usually consists of a quick stroking or rotary massage. Inhibition consists of slow, steady pressures, often applied with stretching of the underlying or adjacent tissues."2 Sato demonstrated this phenomenon with somato-endocrine reflexes.54 Pinching stimulation of the lower chest of the anesthetized rat increases the rate of secretion of adrenaline and noradrenaline by the adrenal medulla. In contrast, innocuous brushing of the same surface area decreases the rate of secretion. Barber indicated that "with a thorough knowledge of the various nervecenters, and the innervation of the different tissues and organs, the osteopath is able to coordinate the nerve-force of the body. He can increase the nerve-current to almost any part of the being, and can quiet an excessive one as well."5 A second technique to accomplish coordination, which needs further researching, may date to the influence of what historically has been called "magnetic healing" in the practice of osteopathy. It involves holding the practitioner's hands over certain spinal centers at the completion of treatment to coordinate them rhythmically. The harmonizing of coupled oscillators into a single, dominant frequency is frequency-selective entrainment. Skilled practitioners may enhance this transfer with the use of empathetic, meditative, centered states.33 Control theory may help us better understand coordination
within the body. A control system is a connection of elements that
communicate with each other to produce a specific effect. Control
systems with negative feedback regulate; those with a positive feedback
system do not regulate but can disrupt the status quo.31
An example of the former are the muscle spindles that control postural
balance, and an example of the latter is the tickle in one's throat that
can produce reflexive coughing.
Centers The concept of centers is inherent in the osteopathic
model of treatment. From the beginning of the profession, osteopathy
recognized the significance of certain nerve ganglia as important centers
that influence and regulate the vital processes of the body such as circulation,
assimilation, and elimination. Barber (1898) states:
We all agree upon the one great point, that man is a machine, and that nerve-centers have been discovered upon which a pressure of the hand will cause the heart to slow or quicken its action, from which we can regulate the action of the stomach, bowels, liver, pancreas, kidneys, and the diaphragm. The thousands of people snatched from the grave by an application of these never-failing principles are proof positive that at last the keynote has been struck; and a school [osteopathy] established that can explain intelligently why certain manipulations produce certain results.5The early osteopaths found a number of locations along the spine whereby the physiology of specific viscera could be affected by stimulation or inhibition of the center. According to Tasker (1903): An osteopathic center is that point on the surface of the body which has been demonstrated to be in closest central connection with a physiological center, or over the course of a governing nerve bundle. No portion of the nervous system ever functions absolutely independently. The action of every portion affects all other portions, but certain areas in the brain and spinal cord seem to be somewhat set apart to govern or coordinate the physiological activity of certain organs. Physiology has demonstrated a large number of these centers.60Many centers correspond to locations on the chain of sympathetic ganglia, from which nerves go to the viscera. Different books give different numbers of centers. For example, Ashmore identified primary and secondary centers.2 Korr diagrams the centers along the spine, with connections to the viscera.28 There are areas in the cervical, upper thoracic, mid-thoracic, and lumbar regions where the ganglia are fused: C2-3, T4, T9, and L4. Cayce indicated that these may be especially important regulatory centers in the coordination between sympathetic and central nervous systems.36 An example of treating one of the centers, using
an inhibitory technique as discussed in the coordination section above,
is shown in Figure 3.
Drainage and Circulation Like the concepts of centers and reflexes, the concept of drainage dates back to the early days of osteopathy. Riggs (1901), in a textbook section entitled "Brain Troubles," states: The osteopath's work is directed toward toward two primary objects: First. The equalizing of the general circulation of the blood. Second. The continued control of the blood supply to the brain and correlative drainage. To accomplish these ends the circulatory centers are first thoroughly treated; the muscles, ligaments and tissues which surround them are relaxed by movements which will stretch the tissues. The next treatment is a stimulation put upon the deeper structures so as to secure the action of the heart and arteries.51Numerous techniques are given in osteopathic texts for controlling circulation and drainage. Chapman's reflexes are one example that has already been mentioned. Kuchera also gives ideas for detailed treatment of lymphatic system dysfunction. The three basic goals are:
There is no argument about the importance of maintaining lymphatic flow from the lungs in disease or in health. Basic research, as well as medical and osteopathic research, has proven that chronic lymphatic congestion with resultant poor oxygenation of the cells is associated with increased infection, increased mortality, increased healing time, and increased fibrosis and scarring if healing does occur. Studies have shown that tissue congestion decreases the effectiveness of medical therapy. Respiratory therapy, pulmonary toilet and osteopathic manipulative treatment all have substantial effect on the prognosis of a patient with a respiratory infection when their inclusion is applied to enhance homeostasis.30Thoracic lymphatic and splenic pump techniques have proven especially useful, as discussed in the research section below. Similarly, in glaucoma, the buildup of pressure has been linked to poor lymphatic drainage of the eye. "Where the sclera, cornea, iris and ligamentum pectinatum meet is defined as the angle of the anterior chamber of the eye. 'Upon the integrity of this angle depends the proper circulation of lymph to nourish the anterior portion of the eye;' glaucomatous changes have frequently been linked to poor lymphatic drainage of the eye."62 The four key concepts can be used for specific therapeutic
purposes or as part of a general treatment. A description of a general
treatment described by Barber in 1898 is provided in Table
2. A good general treatment has been considered a tonic to the
overall system, stimulating the nervous and circulatory systems.
It requires about 20 minutes.17
RESEARCH ON PHYSIOLOGIC REGULATION Research on physiologic regulation is scattered through the osteopathic, chiropractic, and massage literature. Selected studies demonstrating regulation of a variety of body systems are included here. The studies vary from clinical case reports to double-blind, controlled experiments. Much research has been done on the thoracic lymphatic pump, a technique that regulates circulation and drainage. The use of lymphatic pump techniques goes back to the early days of osteopathy.38 The thoracic lymphatic pump has been shown to modify immune function24,34,35,46 and to improve respiratory function.7,56 Wallace et al. provide a good overview of the lymphatic pump.61a Measel cites several studies from 1910 to 1934 demonstrating an effect of osteopathic stimulation of the spleen on immune function.34 Measel investigated the effect of the lymphatic pump on the immune response of normal male medical students. He used two serologic tests to assess immune response to pneumococcal polysaccharide as an antigen. The lymphatic pump group had a statistically greater immune response than the control group, which received no treatment. In a later, double-blind study, Measel and Kafity demonstrated a significant change in bone marrow (B) and thymic (T) derived cells in peripheral blood, with the lymphatic pump technique.35 Jackson et al. explored the effect of lymphatic and splenic pump techniques on the antibody response to hepatitis B vaccine.24 The experimental subjects (n = 20) received the lymphatic and splenic pump procedures three times per week for 2 weeks after each vaccination. The control subjects (n = 19) received vaccine but no osteopathic manipulative therapy (OMT). Fifty percent of the subjects in the treatment group achieved protective antibody titers on the 13th week; only 16% of the control subjects had positive antibody responses. This is further evidence that the lymphatic and splenic pumps enhance immune response. Sleszynski and Kelso explored the value of the lymphatic
pump in alleviating respiratory distress following abdominal surgery.56
They compared two 21-patient groups of postoperative cholecystectomy patients
in a 1-year, randomized, researcher-blinded trial. Patients treated
with the thoracic lymphatic pump (TLP) technique had an earlier recovery
and quicker return to preoperative values of two respiratory parameters
than patients treated with incentive spirometry, a
A particularly interesting historical study cited by Kuchera and Kuchera looked at the outcomes from conventional medical therapy compared with OMT in the flu epidemic of 1918: The effectiveness of osteopathic manipulative support for patients who were not receiving effective medications was clinically tested during the flu epidemic of 1918. Antibiotics had not yet been discovered to help patients fight bacterial complications. Even today, antibiotics are ineffective against viral infections. In this study of 100,000 people with influenza, Smith reported that patients who received osteopathic manipulation had a 0.25% overall mortality and a 10% mortality rate if they developed pneumonia. The mortality rates for patients who only received medical care and no osteopathic manipulation were 5% overall and 30-60% if they developed pneumonia.30A number of studies have shown the effectiveness of manual therapy in modifying respiratory physiology. Stiles, for example, looked at chronic obstructive pulmonary disease.59 Jackson and Steele reviewed the literature on the osteopathic manipulative treatment of asthma.23a They found studies dating back to the 1920s in which OMT was effective in producing physiologic changes in asthma patients. Manipulations included cranial flexion, the thoracic lymphatic pump, and spinal manipulation. Some recent articles on the physiology of asthma lead us to suggest that historical osteopathic techniques for influencing both the sympathetic and parasympathetic nervous systems may be useful in treating asthma.10a,24a,25a,25b,30b,55a In another study involving the respiratory system, Belcastro et al. explored the use of OMT in treating wheezing due to bronchiolitis in infants.7 The OMT included scapular release, rib raising, intercostal fascial release, diaphragm release, and cranial fascial release. Because of the small number of subjects (12) and the absence of a control group, it was not possible to determine the efficacy of the treatment. Nevertheless, the authors are optimistic that, with transcutaneous oxygen measurements, the value of this form of OMT on respiratory physiology could be determined. Radjieski et al. conducted a study of the effects
of osteopathic manipulative treatment on patients with pancreatitis.48
The study was randomized with a control group and with the attending physicians
blind to group assignment. The treatment involved 10-20 minutes daily
of a standardized protocol using myofascial release, soft tissue, and strain-counterstrain
techniques. Patients who received OMT averaged significantly fewer
days in the hospital before discharge (mean reduction,
The early osteopaths made much of the ability of
manual therapy to affect the cardiovascular system. In modern research,
Rogers and Rogers have reported that osteopathic manipulative therapy is
of significant value in some patients with coronary insufficiency.52
Burchett et al. found that manual therapy in the form of generalized paraspinal
inhibition is useful in decreasing
Hypertension is also amenable to manual therapy and
is a condition for which there are reports going back to the early days
of osteopathy.12 Mannino3l and Northrup42
have shown substantial drops in blood pressure with osteopathic manipulative
therapy. In the Mannino study of hypertensive patients, treatment
of Chapman's posterior points to the adrenals resulted in a
Mannino looked at both systemic blood pressure and serum aldosterone levels in hypertensive patients.31 It is possible that abnormal function of the angiotensin-aldosterone system may be involved in some forms of hypertension. No significant alterations of systemic blood pressure were demonstrated, but there was a significant, reproducible decrease in serum aldosterone levels after osteopathic manipulative therapy. Mannino speculated that insufficient time was allowed for the hormonal change to affect blood pressure. Morgan et al. also attempted to use spinal manipulation
to influence hypertension.40 They employed a different
manipulative technique than Mannino did (a spinal manipulation/soft tissue
massage) to lower blood pressure on the principle that major autonomic
outflows are present at the chosen locations. They did not find evidence
of effectiveness of their technique but noted
Regulatory techniques in the head and neck area have also been studied. Purdy et al. demonstrated that gentle, soft tissue manipulation in the suboccipital region can result in significant changes in blood flow in the fingers, mediated by the sympathetic nervous system.47 Their result is particularly interesting because it demonstrates measurable changes in the autonomic periphery during manipulation of a dermatome unrelated to the area being measured. This shows the complexity of reflexes that may be used in physiologic regulation. Craniosacral technique focuses primarily on the head.
The goals of craniosacral technique include improving circulation and venous
drainage. Central to craniosacral therapy is the concept of the articular
mobility of the bones of the cranium. The relationship between craniosacral
dysfunction and symptoms has not been established firmly in controlled
studies.18 Nevertheless, Greenman et al. cite several
clinical studies suggesting a relationship. Of particular interest
is an efficacy study of
Kaluza and Sherbin performed a controlled study of
the physiologic response of the nose, utilizing osteopathic manipulative
treatments They took a systen-fic and historical approach to the importance
of the nose in general body physiology, stating: "If a therapeutic modality
is capable of improving nasal function, it is then implied that the body
as a functioning unit is also improved."26 They noted
that there are a number of reflexes involving the nose, including both
sympathetic and
Misischia39 and Feely et al.13 have shown that osteopathic manipulation can be effective in reducing intraocular pressure in glaucoma. The Feely study was a double-blind, randomized study that reported significant pressure changes after osteopathic manipulative therapy. In a placebo-controlled study, Guthrie and Martin
demonstrated that inhibitory pressure in the lumbar area was effective
in relieving pain during labor, whereas thoracic pressure was not.21
The Continuum of Manual Therapy for Regulation Specific adjustments have been, and will likely continue to be, the province of specialists, e.g., osteopaths and chiropractors. For regulation, on the other hand, there is a continuum of manual therapy. The early osteopaths did both, and some felt that this distinguished them from chiropractors, who focused on specific adjustments. Few modem osteopaths concern themselves with regulation, although it is of great importance to some.30 But regulation is not limited to osteopaths. There is a continuum related to the degree of training in regulation. Manual therapists who employ techniques of regulation include physical therapists, massage therapists, nurses, and some chiropractors. Acupressure, acupuncture, and manual lymph drainage would also fall in the area of regulation. For example, the protocol followed by Kaluza and Sherbin for improving nasal drainage did not involve any form of spinal manipulation or adjustments. It consisted of soft tissue work around the face, including massage. Similarly, the soft tissue work used as simulated chiropractic manipulation in the Balon et al. study enhanced peak expiratory flow in asthmatic children.4 Guthrie notes that his technique of lumbar pressure
to relieve pain during childbirth does not require an osteopath; it may
be administered easily by a husband or other nonprofessional.20
Similarly, Sleszynski and Kelso state that the thoracic lymphatic pump
technique (used in this case for postsurgical respiratory problems) can
be taught to and administered by a respiratory
Of particular interest is the physiotherapist Harold
Reilly, who originally was trained as a chiropractor but later developed
many regulatory techniques.49 Reilly integrated massage
with chiropractic and osteopathic concepts to yield a broad-based system
of manual therapy. For more than 30 years, the Reilly Health Institute
in Rockefeller Center in New York City was a health mecca for prominent
people. Reilly combined traditional massage with "rotations," the
manipulation of the long bones of the body, with a variety of drainage
techniques, and with hydrotherapies such as fume baths, sitz baths, and
colonic irrigations, all to affect the physiology of the patient.
Reilly's approach continues to be taught at the Reilly School of Massotherapy
in Virginia Beach. There are also other specialties of manual therapies
that are no longer practiced, such as neuropathy and spondylotherapy, which
employed regulatory techniques.
DIRECTIONS FOR THE FUTURE
Research on Regulatory Techniques There is a wealth of regulatory techniques in the works of such authors as Barber and Hazzard that are not in common use today and have never been scientifically studied. Basic research into the anatomy and physiology of manual therapy effects is needed to explain the relationship among structure and function, specific techniques, and biologic effects. For example, there is a need for a systematic investigation of both centers and reflexes (e.g., Chapman's reflexes). There is also a need for clinical demonstration of the effectiveness or ineffectiveness and under which conditions techniques such as Barber's can be effective. To accomplish these goals, several considerations
might be helpful. First, it is necessary to acknowledge the full
spectrum of manual therapies. This will help with developing research
methodology that addresses the problem of active control treatments that
distort findings and can compromise conclusions. Second, whenever
possible, the political turf battles within manual
Many feel that we are in the midst of a medical revolution. There
is currently a window of opportunity to legitimize these techniques and
educate the medical establishment of their efficacy.
REFERENCES 1 .[Reference deleted.]
TABLE 1. Relationship between Spine Segments and Internal Organs
TABLE 2. General Osteopathic Treatment 1 . Place the patient on the side; beginning at the upper cervicals, move the muscles upward and outward, gently but very deep, the entire length of the spinal column, being very particular in all regions which appear tender to the touch, have an abnormal temperature, or where the muscles seem to be in a knotty, cord-like, or contracted condition. Treat the opposite side in a similar manner. 2. With the patient on the back, place the hand lightly over the following organs, vibrating each two minutes, respectively: lungs, stomach, liver, pancreas, and kidneys. 3. Flex the lower limbs, one at a time, against the abdomen, abducting the knee, and abducting the foot, strongly as the limb is extended with a light jerk. 4. Grasping the limb around the thigh with both hands, move the muscles very deeply from side to side the entire length of the limb. Treat the opposite limb in a similar manner. 5. Place one hand upon the patient's shoulder, pressing the muscles down toward the point of the acromion process; with the disengaged hand grasp the patient's elbow, rotating the arm around the head. 6. Holding the arm firmly with one hand, with the other rotate the muscles very deep the entire length of the arm; also grasp the hand, placing the disengaged hand under the axilla, and give strong extension. Treat the opposite arm in a similar manner. 7. Place one hand under the chin, the other under the occipital, and give gentle but strong extension. 8. Place one hand under the chin, drawing the head backward and to the side; with the disengaged hand manipulate the muscles which are thrown upon a strain. Treat the opposite side in a similar manner. Also manipulate, thoroughly and deep, the muscles in front of the neck. 9. Place the patient upon a stool; the operator placing the thumbs upon
the angles of the second fibs, an assistant rising the arms slowly but
strongly above the head as the patient inhales; press hard with the thumbs
as the arms are lowered with a backward motion, patient relaxing all muscles
and permitting elbows to bend; move the thumbs downward to the next lower
ribs; raise the
From Barber ED: Osteopathy Complete. Kansas City, MO, Hudson-Kimberly Publishing, 1898, pp 306-307.
|